



How has this happened?
Birthing two big babies vaginally over a decade ago has finally backfired on me. It’s been a slow burn, with bumps along the path that have led me to a diagnosis of mixed urinary incontinence. It shouldn’t come as too much of a surprise because I experienced extreme fecal urgency shortly after having my first son. He was born weighing a mighty 9lbs 6oz, and required an episiotomy, where the doctor took a pair of scissors to my perineum to dislodge him from my birth canal. I had begged them not to. Being a hyper independent woman, I wanted to “do it alone”, which I could have done, had the maternity staff not insisted on relocating me when I was already in transition from a pool for labouring mothers into a stark clinical birthing room.
Their interference stalled my progress, leading to me feeling emotionally unsafe. Repeatedly I asked them if I had pooed myself yet, since I had learnt during antenatal classes that this was a natural sign that the baby’s birth was progressing. I had wanted to poo myself, but they misread this repetitive question for paranoia, anxiety, or something else that I should not have been made to feel in my vulnerable state.
Everything slowed down to almost a standstill, and I ended up being instructed to lay flat on my back, feet in stirrups being told to “Push him out of your bottom!” Really it was all a recipe for fecal incontinence, and I have done well to recover especially considering that my GP at the time dismissed this as normal.
Baby two born three years later was even heavier at 9lbs 12oz. I water-birthed him at home as an active resistance to unnecessarily over-medicalising his birth. This time around I tore, and stitches healed well after both births.
My youngest was almost born in the downstairs toilet, as I was able to completely relax my pelvic floor muscles whilst sitting there, and felt the most comfort in a very uncomfortable situation.

What is wrong with me now?
Vaginal childbirth is often a contributing factor to later developing bladder incontinence, which seems to be the case for me. Leaking urine didn't really start until my kids became enthusiastic about playing on trampolines, and I wanted to get involved. Going for a wee right before a bounce was not enough to prevent me weeing again immediately mid-bounce. That was a few years ago, and I now know to stay well away from trampolines.
My avoidance served me well again for a while, but very recently the leaking has become regular and with less obvious reason.
I tried ignoring it and hoping it would just stop.
It didn't.
So I tried wearing period undies and thinking I could get away with it.
Because everyone complains about leaking sometimes, right? A sneeze or a cough can be a common and seemingly unavoidable trigger.
Besides, my advertising algorithm is now full of curvy, happy midlife women wearing incontinence pads and living their best lives!
I thought it was normal and I just had to put up with it. Although my keen sense of smell meant that I would worry that I smelled of urine. It is one thing to know I have this problem without other people knowing about it too!
But then the leaking started happening during my twice weekly personal training sessions. I love working with my trainer, and I told her what was going on. I started following the programme she set me to strengthen, and learn to relax, my pelvic floor.
Last Friday it got so bad that I was leaking during the training sessions actively intended to stem the flow. What was wrong with me?
Reverse lunge, drip.
Reverse lunge, drip.
Reverse lunge, drip.
Luckily that was the same day that I was seeing the gynaecologist to self-advocate for my hysterectomy. The approval granted for the surgery was a huge weight off my mind, yet the weight of my burgeoning bladder persisted. The gynaecologist internally assessed me and diagnosed a stage one pelvic organ prolapse.
Finally, I had an acceptable explanation for my urinary incontinence. It was a medical issue and not a moral failing on my part. I could live with that, and I found it oddly reassuring.
All weekend I wondered if the prolapse could soon be repaired surgically during my upcoming hysterectomy. I felt vindicated in my urine leaking pattern - of course I was leaking if I had a prolapse. The prolapse must have occurred whilst birthing my baby boys, and I was asymptomatic until now.
But then I worried that the surgery could in fact exacerbate the pelvic organ prolapse, worsening my bladder control. I knew I needed to be proactive in managing this condition, after listening to a great podcast episode on the topic:
Why see a pelvic health physiotherapist?
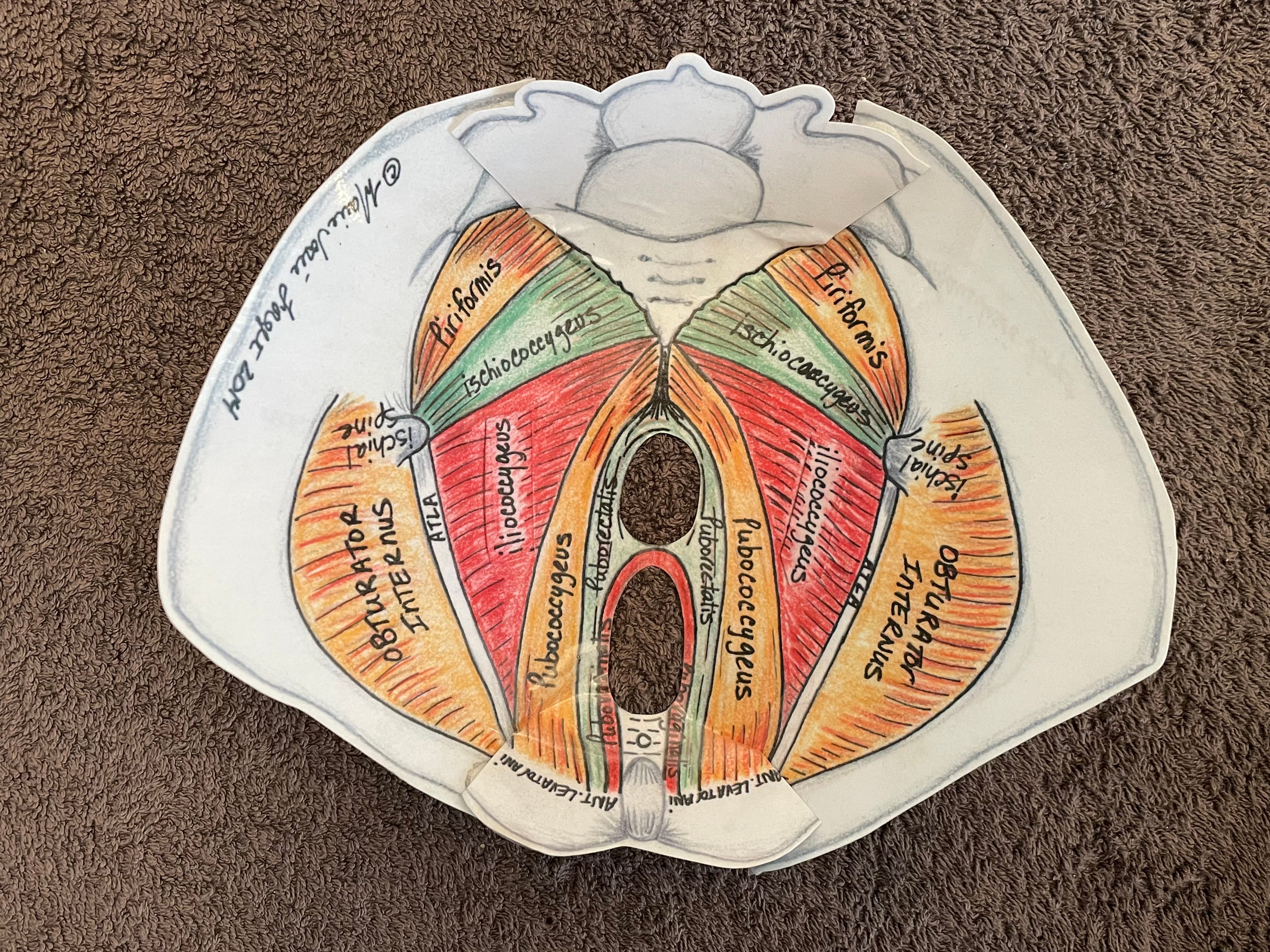
Here is a good visual explanation of what the female pelvic floor is and why it matters:
Physiotherapist Fiona Rogers talks us through what the pelvic floor is and how it works.
Do you know how to do a pelvic floor exercise properly or have you been taught to just suck everything up and in? Watch here how to do it properly.
Fiona firmly believes if you understand where the muscles are and how they work then you are more likely to understand and learn how to exercise them properly.
Credit: Pelvic Floor Exercise
Hormonal changes during menopause can significantly impact the pelvic floor muscles, contributing to symptoms such as urinary incontinence, vaginal wall prolapse, and sexual dysfunction.
A pelvic health physiotherapist can assess for muscle weakness, overactivity, or imbalance and develop individualised treatment plans. Interventions may include physiotherapy-guided pelvic floor muscle training, manual therapy, biofeedback, and structured relaxation techniques.
These strategies are designed to restore muscular strength, coordination, and neuromuscular control, which supports continence, vaginal wall integrity, and overall pelvic health.
Credit: Positive Pelvic Health
Already armed with some basic information on my new hyper fixation, I reached out to Jennifer Dutton of Positive Pelvic Health. Jennifer is a pelvic floor physiotherapist who had been highly recommended to me. Amazingly, she offered me a cancellation for an in person initial consultation the very next day.
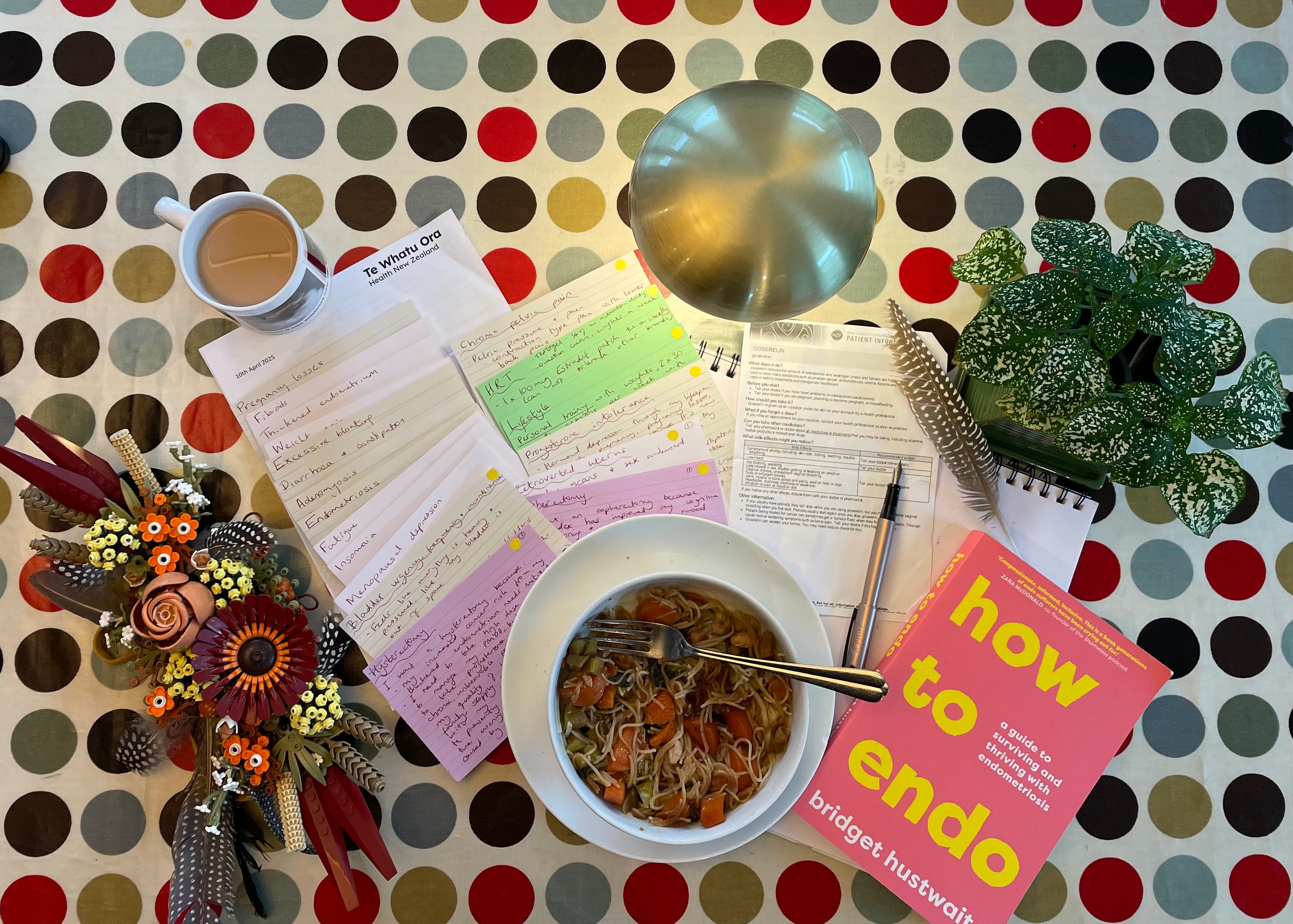
Knowing that verbally retelling my medical issues is overwhelming for me, I brought along the notes I had prepared for the gynaecologist appointment. Jennifer took a very thorough medical background and was empathetic and reassuring.
Upon internal examination, both standing and lying down, Jennifer said there was no pelvic organ prolapse present. She explained that vaginas and other organs supported by the pelvic floor will show natural signs of aging in midlife, as our skin loses collagen and oestrogen, also evidenced externally by how our faces, breasts and stomachs may also sag.
Here is a video of Jennifer being interviewed about pelvic health, where she explains much of what she told me during my appointment:
I wonder if the gynaecologists see any saggy vaginas in their medical training, as mine obviously can’t be a textbook model anymore!
With my newly undiagnosed pelvic floor prolapse, I was able to spiral into a new panic about whether indeed my urinary incontinence was just a moral failing on my part after all…
What is urinary incontinence?
My current issues, known individually as urge incontinence and stress incontinence, together create a combined diagnosis referred to as mixed incontinence. Yay.
Urinary incontinence is the unintentional passing of urine. It's a common problem thought to affect millions of people.
There are several types of urinary incontinence, including:
stress incontinence – when urine leaks out at times when your bladder is under pressure; for example, when you cough or laugh
urge (urgency) incontinence – when urine leaks as you feel a sudden, intense urge to pee, or soon afterwards
overflow incontinence (chronic urinary retention) – when you're unable to fully empty your bladder, which causes frequent leaking
total incontinence – when your bladder cannot store any urine at all, which causes you to pass urine constantly or have frequent leaking
It's also possible to have a mixture of both stress and urge urinary incontinence.

Autism, Interoception and Adult Incontinence
So I am leaking on the regular, and trying not to blame myself for this recurring issue.
It is so normalised yet hidden. TV ads for pads and absorbent pants proliferate, subtly telling us it is okay to leak urine, as long as nobody else knows.
Well, fuck that shit! When I leak, I tell everyone about it. Part of my neurodivergent profile has been a lifelong shamelessness. I don’t feel a need to hide anything. I refuse to feel shame and embarassment for urinary incontinence, despite having a niggling sense of regret that it is happening to me.
Urinary incontinence is just another social taboo to stack on top of all the others I make it my mission to bust.
Why would being autistic affect my urinary continence? Especially seeing as I am not aware of having any intellectual disability which may be more likely to co-occur with toileting issues. If anything, before perimenopause I may have been considered intellectually gifted. Yet my cognition has declined in this life phase, and I cling to the hope that this regression is temporary and reversible.
Interoception is our capacity to identify our internal states and needs. When this is reduced, as mine has been in perimenopause, and is combined with a regression in executive functioning skills, then noticing when I need to use the toilet, and acting on the urge, can lead to me not responding accordingly.
Interoception
Receptors on our internal organs are responsible for interoception signals that provide information on our internal body and emotional states.
Experiences: urge to urinate, hunger, temperature, pain, sadness, joy, anxiety.
Interoceptive Over-Responsivity
With interoception over-responsivity the person feels too much of their internal signals. They “over-feel” their internal sensations. Signs of over-responsivity include:
Visits the nurse’s office several times a week with aches, pains, and illness
Requests frequent bathroom breaks
Limps on an injured knee or ankle for longer than expected
Credit: Dr Megan Anna Neff at Neurodivergent Insights blog post What is Interoception and How to Improve Yours
It seems that my extremely frequent and protracted toilet visits may be down to interoceptive over-responsivity. I have developed an overuse of the toilet that has led to me missing appropriate bodily cues as to when I need to use the bathroom. Unfortunately, this has been the case day and night, and may be a contributing factor to my insomnia.
Many of us may have experienced differences in toileting from our neurotypical peers as children, and/or have supported our own neurodivergent children with delayed or fluctuating bladder and bowel control. Neurodivergent people with co-occuring intellectual disabilities may be more likely than those without them to face toileting differences through adolescence and adulthood.
I had never anticipated making what I consider in myself to be significant self-care regressions in perimenopause and now continuing into my hormone blocker induced medical menopause. Nobody had ever talked to me about urinary incontinence, as it is such a taboo topic. Until it became an issue in my daily life, it wasn’t forefront of my mind.
Yet it would seem that the menopause transition, like during puberty, is a time of developmental shifts and changes. In our capitalist patriarchal society (at least where I live), we are told we should be ever evolving upwards. Improving. Making our lives better for ourselves. Regression is culturally unacceptable and often shunned. So there is little wonder why people mask their incontinence as they age, for fear it could be interpreted as a sign of weakness.
As I have been writing for over a year now, The Autistic Perimenopause: A Temporary Regression aims to highlight a common perception for many of our neurokin that this life phase characterised by extreme hormonal flux can lead to regressions and changes in our cognition, energy, emotional regulation, sleep, metabolism and so on.
If we conceptualise the spectrum that is autism as a state of constant flux through the lifespan within our social communication, energy, interests, sensory regulation etc. where we can dynamically change in capacity from day to day, or hour to hour, then perhaps it would stand to reason that our interoception and even urinary continence can oscillate over time.
It seems from a quick online search that my anti-anxiety medication, Setraline, has urinary incontinence as a known side effect. I started to take it when first diagnosed autistic and highly anxious, as I was unwittingly entering perimenopause, and my kids were asking me to use the trampoline with them often. What a perfect storm! 💦
Progesterone intolerance may also be contributing to my urinary incontinence. I have to take progesterone alongside oestrogen in my HRT regimen until I have a total hysterectomy, because progesterone mitigates the potential cancer risk of taking oestrogen. Not only is my progesterone intolerance causing bloating, depression, suicidal ideation at times, but now it may also be counteracting the potential benefits of oestrogen on maintaining my urinary continence.
Menopause and Incontinence
The scale of female urinary incontinence is extreme yet it remains a taboo topic.
According to Liz Earle, it takes women 12 years on average of experiencing urinary incontinence symptoms before feeling able to talk to their family doctor. It then takes another two years before they decide to book a doctor’s appointment. Then for many women, their symptoms are dismissed by their doctor.
Liz Earle interviewed uroligist (bladder specialist) Dr Vik Khuller on the impact of bladder issues, and he said that “Women suffer in silence… But don’t have to put up with it.” Dr Khuller also discussed the prevalence of bladder and pelvic organ issues in women who have joint hypermobility and/or Ehlers Danlos Syndrome. They also discuss mast cell activation syndrome (MCAS) and “Covid bladder” in this succinct and informative podcast episode:
Urinary symptoms are part of the umbrella term genitourinary syndrome of the menopause (GSM), when it occurs due to fluctuating and declining oestrogen levels in perimenopause and beyond.
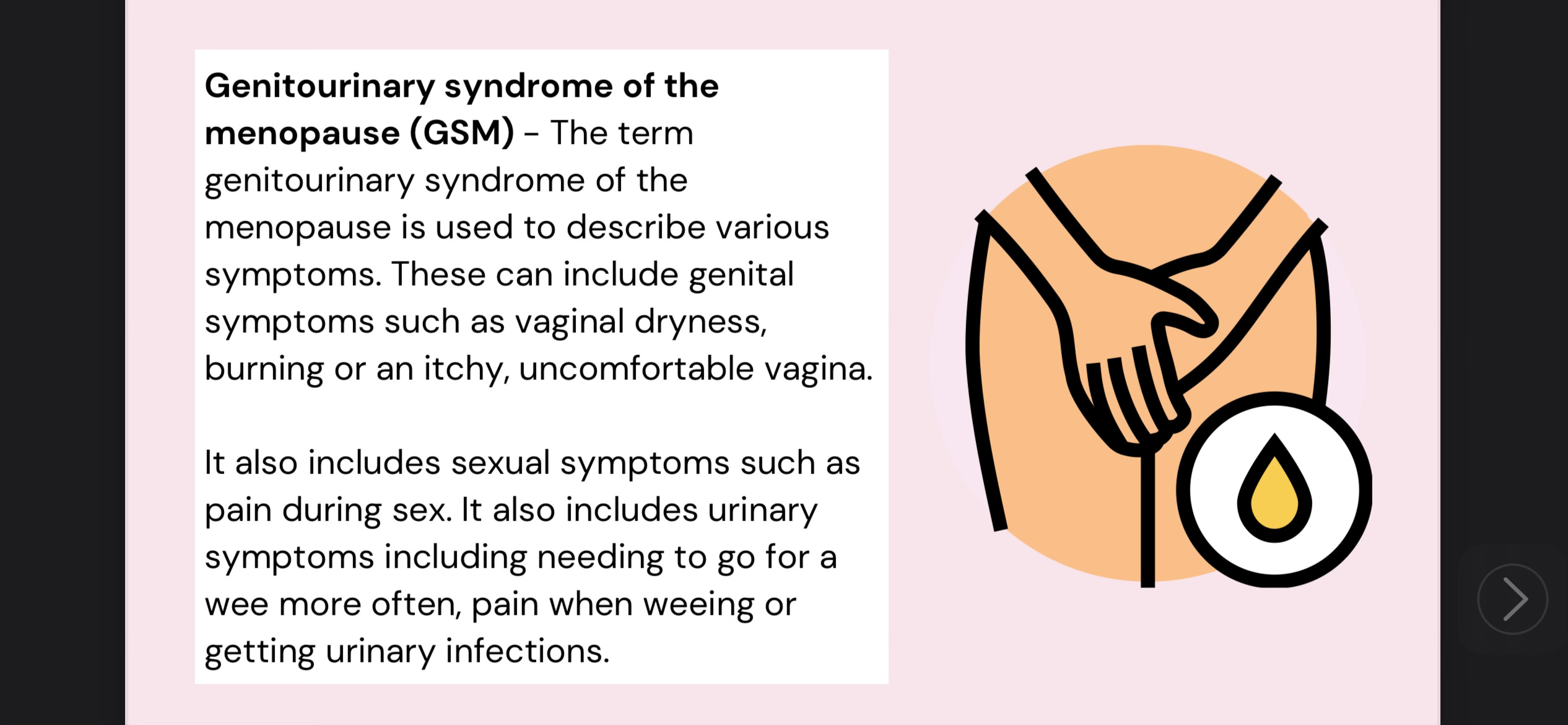
Vaginal oestrogen creams and pessaries can be prescribed to add localised oestrogen back into the area. It is a good option for people who can’t or don’t want to take systemic HRT. It can improve bladder symptoms, vaginal atrophy, vaginal dryness and reduce occurences of urinary tract infections.
The Australasian Menopause Society provide further and in depth information in the information booklet entitled, Genitourinary Syndrome of Menopause.
Here is an article I wrote last year about vaginal atrophy:
When is a vagina not a vagina? When it’s A Trophy! 🏆

Autistic people feel things deeply to our very core, to our bones. We can sometimes hear the rush of our own blood coursing through our veins. Feel our heartbeat thumping in our throats. Hear ourselves chewing our food and think we are deafening everyone around us for miles and miles and miles. Hear other people chewing…

What to do if you are experiencing incontinence
In Menopause and Urinary Incontinence, Healthline advise, “You don’t have to accept occasional bladder leakage as another side effect of menopause or aging. In many cases, there are things you can do to stop and even prevent urinary incontinence… Speak with your doctor to learn more about your condition, treatment options, and outlook.”
Different treatments are necessary according to what may be causing urinary incontinence in different people. There is no one size fits all treatment plan, but please do not feel embarassed about it. Go and discuss it with your doctor. They will have heard it all before and can make an appropriate referral, and/or advise on the next best steps to help you.
However, should you feel your doctor has dismissed you, that you have medical trauma, or are reluctant to discuss this with your family doctor, perhaps your first step could be to speak to a local pelvic health physiotherapist.
In addition, you may like to research the topic further at:
International Urogynecological Association
International Continence Society
Strengthening and relaxing the pelvic floor is key
Pelvic health physiotherapist Jennifer Dutton said that, as in my case, pelvic organ prolapse is commonly overdiagnosed, and that recent guidelines advise healthcare practitioners not to tell a woman if she has a stage one pelvic organ prolapse. She said it can create unnecessary concern and, rather, women should be supported to follow an appropriate treatment plan, not feel like they have a medical diagnosis that they are unable to improve.
Jennifer also told me that many women have urge and stress incontinence due to tension in the pelvic floor, not weakness as we are always led to believe. So when we are told just to keep doing Kegels or pelvic floor strengthening exercises, it can often make matters worse not better.
The plan she has created for me is designed to relax the tension in my pelvic floor muscles, and even out overall strength so that the different parts work together rather than against each other.
This includes:
full body massage
using a Shakti mat daily
diaphragmatic breathing
foam rolling my upper legs and mid spine
trigger point spiky ball massage for my glutes
In addition, to cut all caffeine as it is a bladder irritant, and to improve my insomnia. This is already having a marked effect only four days in! I had a caffeine withdrawal headache the first day, but no negative effects thereafter.

Coincidentally I started taking non-stimulant Clonidine alongside my ADHD stimulant Vyvanse last week in order to help overcome my insomnia, and to reduce my high blood pressure. Alongside cutting caffeine and introducing relaxing lifestyle changes, this should all be helping improve my overall health and wellbeing. I hope!
Bladder retraining techniques have also been explained by Jennifer, and these are difficult to manage during the daytime, but at night I am no longer being frequently woken up by my overactive bladder. This is life changing!
Bladder training
Bladder training involves changing habits. It means going to the toilet at set times, even when there's no urge to urinate. If the times between urinating increase little by little, the bladder fills more fully. This helps control the urge to urinate.
A bladder-training program often follows these basic steps:
Find the pattern. Keep a diary for a few days. Jot down every time you urinate. A health care provider can use this diary to help you make a schedule for bladder training.
Wait longer before urinating. Your bladder diary can tell you how long you wait between urinating. Add on 15 minutes. If you usually urinate every hour, try to wait for an hour and 15 minutes.
Little by little, increase the time between trips to the toilet until you can wait 2 to 4 hours between trips. Increasing the time slowly gives the best chance for success.
Stick to the schedule. Once you've made a schedule, do your best to stick to it. Urinate right after waking up in the morning. And urinate each scheduled time even if you have no urge to go.
If you have an urge but it's not time to go, try to wait. Distract yourself or use ways to relax, such as deep breathing. If you feel you're going to have an accident, go to the toilet. But then return to the schedule.
Don't give up if you don't succeed the first few times. Keep trying. Your control is likely to increase.
Credit: Mayo Clinic’s Bladder Control: Lifestyle strategies ease problems
I now have a two hourly timer on my phone and watch, because part of my neurodivergent presentation is a total inability to sense the passing of time. Every two hours during the daytime, my timer reminds me when I can go to the toilet, and not before!
I am building up to managing 3-4 hourly trips before I see my physio Jennifer again in around 6 weeks time.
Wish me luck! 🤞 ⏱️ 🚽 💧 🙌
Cheers,






Share this post